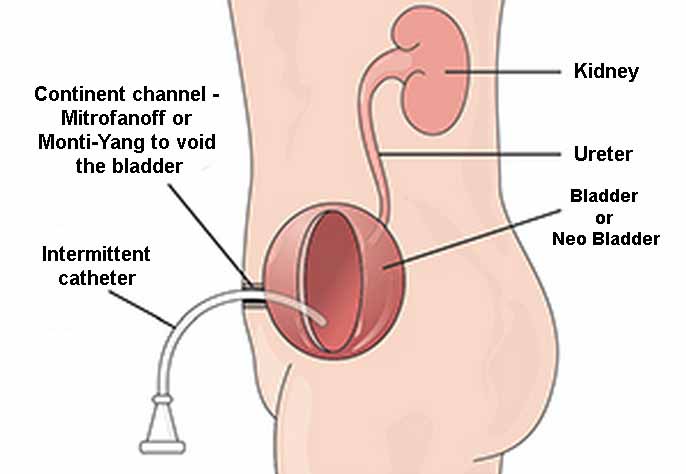
[fusion_dropcap]T[/fusion_dropcap]he Mitrofanoff procedures involves the use of the appendix as a conduit between the bladder and the skin of the abdominal wall when urethral access to the bladder is lost and an alternative route to empty the bladder is required. A catheter is used (usually 4-7 times a day) to empty the bladder. This avoids the need for a long-term stoma bag, which is the more commonly used alternative.
The most important principal of this procedure is the creation of a continent valve in the bladder to prevent urinary leakage between catheterization. This is created by tunnelling the Appendix through the wall of the bladder for a distance of 4-5cm. As the bladder fills the bladder wall is compressed closing the Mitrofanoff tube and preventing leakage.
While The preferred tube for the Mitrofanoff is the appendix, in some cases the appendix may be absent or of insufficient length or diameter to be of use. If this is the case a similar tube can be fashioned from a short segment (2.5cm) of small bowel, which is opened out flat and then rolled to give a longer and narrower tube (5cm length). These Monti-Yang tubes can be joined together to create a sufficient length to bridge the gap between the bladder and the skin.
For many patients the preferred position of the skin into the tube is at the umbilicus. Catheters are then passed through the umbilicus which is hidden from everyday view. Where location at the umbilicus is not possible, the tube is brought out in the lower part of the abdomen below the belt or skirt line.
“Source: Mitrofanoff Australia